
Why is it done?
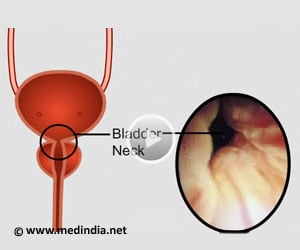
You have a bladder neck contracture or fibrosis
Causes:
- Congenital
- Acquired
Pelvic fractures
Previous TURP/ TUVP
Radical prostatectomy for Prostate Cancer
How is it done
- General anesthetic
- The surgical field is prepared
- A flexible cystoscopy is done to gently dilate the bladder neck and place a small catheter
- A camera port is placed above the Umbilicus
- 3 Additional ports for robotic arms in a horizontal line on the abdomen with 2 assistant ports on the right side of the abdomen
- The abdominal space is entered and the bladder dropped from the abdominal wall.
- Bladder wall is opened at the bladder neck
- Bladder neck opened and scar tissue removed
- YV-flap of bladder mucosa created and advanced into prostatic urethra
- Anterior bladder wall used to close the defect in anterior prostate capsule
- Catheter replaced
- A leak test done
- Drain placed
Post operative care:
- Sutures are subcutaneous and will be dissolved.
- You will have a drain in the wound for 24-48 hours until it drains less than 30ml/24 hours
- You may be discharged on the 2-3 day
- Normal diet will be commenced
Catheter care
- Your catheter will remain for 10 days
- Only after a cystogram (radiological investigations where radio-opaque contrast is placed in the bladder) confirms no leakages from the bladder-urethra-anastomosis, will the catheter be removed
- Remember you will leak initially, with gradual improvement up to 6 weeks post-operatively
- Nursing staff will teach you catheter care
- Your catheter should always be fixed to your leg with a catheter dressing
Complications
- Blood loss < 200 cc
- Wound infections
- The first 6 weeks are the worst with frequency and urgency as a result
- Possibility of bowel injury
Post-operative review:
- Cystogram at 10 days post-operatively to assess complete healing of urethra bladder neck anastomosis to exclude any leakages
- Should there be any leakages, the catheter may remain another 7 days.
- Review in rooms at 6 weeks
- 6 monthly reviews depending on risk factors.
