
Orchidectomy – Radical
Why is it done?
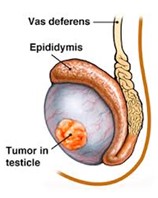
- For testis cancer.
- For testis lesions highly suspicious of testis cancer.
How is it done?
- This is done under general anesthetic.
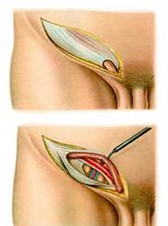
- A single incision is made in the groin. The underlying muscle layers are split for good oncological control.
- The affected testis and spermatic cord are then surgically removed through this incision.
- A metal clip may be left right at the internal inguinal ring, as a future marker, should radiotherapy be required.
- Subcutaneous sutures (which need not be removed) are used, unless stated otherwise.
- A dressing is then applied, which should be removed after 72 hours.
- A local anesthetic is injected into the wound, thus giving post-operative pain relief for the next 4-6 hours.
- A drain may also be left for 24-48 hours to prevent the collection of serous fluids
What to expect after the procedure
- Any anesthetic has its risks, and the anesthetist will explain such risks.
- Bleeding is a common complication. If concerned call the hospital.
- A hematoma (blood collection under the skin) may form and needs to be reviewed as soon as possible.
- An infection of the wound may occur and requires immediate attention.
- Owing to the nature of the surgery and the soft skin of the scrotum, bruising may appear much worse than it is and is no cause for alarm.
- DANGER SIGNS: A scrotum that swells immediately to the size of a football, fever, or pus. Contact Dr Schoeman or the hospital immediately as this occurs in up to 15 % of all cases.
What next?
- The dressing should be kept dry for the initial 72 hours after surgery.
- The dressing should then be removed in a bath. It should be soaked until it comes off with ease.
- The dressing may sometimes adhere to the wound causing slight bleeding on removal. Don’t panic, the bleeding will stop.
- Patients should schedule a follow-up appointment with Dr Schoeman within 2 weeks to review pathology and arrange subsequent management.
- There will be signs of bruising for at least 10 days.
- The suture-line will be hard and indurated for at least 8-10 weeks.
- PLEASE CONTACT THE HOSPITAL DIRECTLY WITH ANY POST-OPERATIVE CONCERNS AND RETURN TO THE HOSPITAL IMMEDIATELY SHOULD THERE BE ANY SIGNS OF SEPSIS.
NB! Regular self-examination highly recommended.
 This is done under general anesthetic.
This is done under general anesthetic.
/Picture148.png) This procedure is done under general anesthetic.
This procedure is done under general anesthetic./Picture146.png)
/Picture147.png)
/Picture149.png) This procedure is done under general anesthetic.
This procedure is done under general anesthetic./Picture152.png)
/Picture150.png)