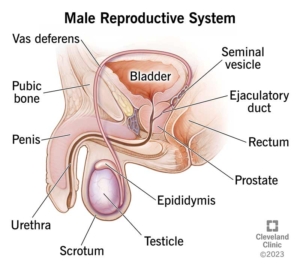
Surgical removal of foreskin with penile block for post-operative pain relief

Why is it done?
- Religious reasons.
- Health reasons.
- Personal reasons.
- Medical reasons:
- Narrowing of foreskin -phimosis.
- Foreskin stuck behind head of penis – paraphimosis.
- Severe infection of the foreskin and head of penis -balanoposthitis.
- Cancer of the foreskin – SCC.
- Trauma.
How is it done?
- This is done under general anesthetic or penile block.
- A cut is made at the level of the glans penis, circumferentially around the penis, through the skin.
- The foreskin is then retracted, and a second incision is made circumferentially around the base of the glans penis.
- The skin between the 2 incisions is then surgically removed.
- Dissolvable sutures are then placed between the 2 remaining edges.
- A Jelonet and Bactroban dressing is then placed tightly around the penis, still allowing urine to pass through the end.
- A local anesthetic is injected into the base of the penis thus giving post-operative pain relief for the next 4-6 hours.
Unfortunately, no infants younger than 12 months can be operated on in any of the private hospitals ONLY at Children’s Hospital.
What to expect after the procedure
- Any anesthetic has its risks, and the anesthetist will explain such risks.
- Bleeding is a common complication.
- With any subsequent erections post operatively, the sutures may pull out causing an opening of the wound with subsequent bleeding.
- An infection of the wound can occur if the dressings are left on too long.
- If the dressing has been applied too tightly, or if there is any discomfort, please remove the dressing immediately. If some hemorrhaging re-occurs, REDO the dressing!
- In very young patients, the foreskin may still be attached to the head of the penis, thus leaving a raw and red glans penis after surgery. Keep the affected area clean and apply ointment as prescribed.
- NB! Each person is unique and for this reason symptoms may vary!
What next?
- The dressing should be removed in a bath 48 hours after the procedure.
- The dressing should be soaked until it comes off with ease.
- The dressing may sometimes adhere to the wound causing slight bleeding on removal. Don’t panic the bleeding will stop.
- As soon as the dressing has been removed, Bactroban (or similar) ointment should be applied on the wound twice a day.
- This may not be required if the foreskin was not adhered to the glans penis.
- On discharge a prescription may be issued for the patient to collect.
- A follow-up appointment should be scheduled to see Dr Schoeman within 2 weeks.
- Please don’t hesitate to direct all pre-operative queries to Dr Schoeman’s rooms.
- PLEASE CONTACT THE HOSPITAL WITH ANY POST-OPERATIVE CONCERNS AND RETURN TO THE HOSPITAL IMMEDIATELY SHOULD THERE BE ANY SIGNS OF SEPSIS.
Download Information Sheet
Wes Circumcision

 This procedure is done under general anesthetic.
This procedure is done under general anesthetic.
 This procedure is done under local or general anaesthetic.
This procedure is done under local or general anaesthetic. This procedure is done at home.
This procedure is done at home.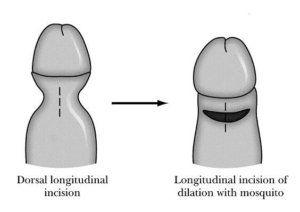
 This is done under general anesthetic or a penile block.
This is done under general anesthetic or a penile block.


 This procedure is done under general anesthetic.
This procedure is done under general anesthetic.