A therapeutic procedure under general anaesthetic, where a rigid cystoscopy is done in the bladder via the urethra, ureteric catheters are placed to enable imaging of the upper tracts with/without insertion or removal of ureteric stents
Why is it done?
To investigate:
- Hematuria (blood in the urine)
- Recurrent upper urinary tract infections
- Space occupying lesions in the kidneys and ureters
- Abnormal cells suggestive of urothelial carcinoma, on urine cytology
Risk factors:
- Strong family history of bladder cancer
- Smokers or passive smokers
- Factory workers: dyes, paints, etc
- Exposure to Schistosoma (Bilharzia)
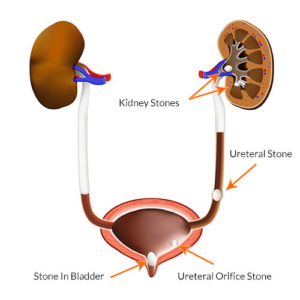
- Renal stone disease, bladder stones
How is it done?
- This is done under General anaesthesia.
- A cystoscopy is performed by placing a camera in the urethra with the help of a lubricant gel and saline irrigation.
- The bladder is then distended with saline.
- The inside of the bladder is viewed for pathology.
- A retrograde pyelogram is done at the same time, (placement of small silicone catheters up the kidney pipes). Through this iodine contrast is injected up into the kidney collecting systems. This facilitates the viewing of kidney pipes and kidney collecting systems on X-ray to exclude any upper tract pathology.
- If any abnormalities are found in the kidney/ ureters, a ureteroscopy (which is the placement of a long thin camera up the ureter) will be performed.
- If any suspicious lesions are seen, a biopsy will be taken.
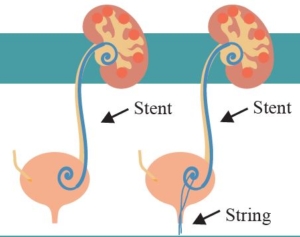
- A ureteric stent may be placed
- Urine would have been sent for cytology, to rule out the existence of cancer.
Antibiotics may be given to prevent infection
Complications
What to expect after the procedure?
- Pain on initial passing of urine
- Bladder infection ranging from a burning sensation to, fever, to puss (rare)
- Bloodstained urine
- Lower abdominal discomfort which will persist for a few days
- Pain radiating from bladder to renal angle associated with urinating.
- An infection could present with a stent being present.
|
|
Indications for a Ureteric stent
· Hematuria from upper tracts
· Dis-obstruction of the ureter caused either calculus, blood clot or tumour
· External compression of the ureter by retro-peritoneal pathology i.e.: Fibrosis, retroperitoneal lymph node compression
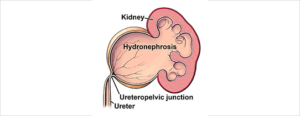
· Reduced renal function associated with hydronephrosis
· Sepsis associated with hydronephrosis |
|
Download Information Sheet
Wes Cystoscopy RGP and Ureteric stents
Copyright 2019 Dr Jo Schoeman

/Picture35.png)

 Patients will receive a general anesthesia.
Patients will receive a general anesthesia.