
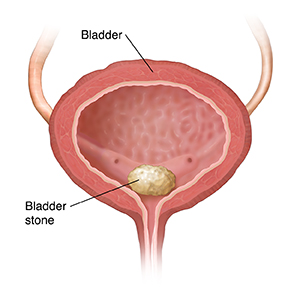
Cysto-Lithopaxy
Endoscopic procedure used for breaking up a bladder stone. Either with a stone crusher or laser
Why is it done?
- To break up a bladder calculus (stone).
Risk factors:
- Bladder outflow obstruction.
- BPH with chronic retention.
- Urethral stricture.
- Neurogenic bladder.
- Renal calculi disease.
- Metabolic disorders.
- Malnutrition.
- Chronic infections.
- Foreign objects in bladder.
How is it done?
- A cystoscopy is performed by placing a camera in the urethra with the help of a lubricant jelly and an irrigate (fluid).
- The bladder is then distended with fluid (saline).
- The inside of the bladder is viewed for pathology.
- If any suspicious lesions are seen, a biopsy will be taken.
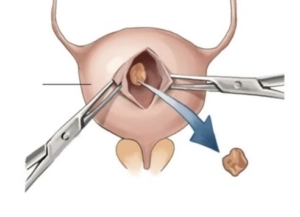
- Stone crushing is attempted with a lithotrite (a crushing device).
- If the calculus is too large, laser will be utilized to fragment the stone and the smaller stones evacuated.
- Antibiotics may be given to prevent infection.


What to expect after the procedure?
- Hematuria (blood in your urine)
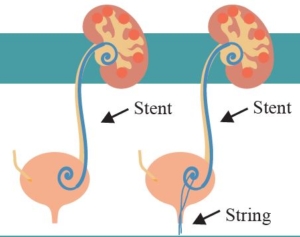
- You will have a n indwelling catheter (IDC), which will remain in your bladder until your urine is clear.
- You may have a continuous bladder irrigation with Saline to help clear the bleeding.
- Pain on initial passing of urine when the catheter is removed.
- Bladder infection ranging from a burning sensation to, fever, to pus (rare).
- Lower abdominal discomfort which will persist for a few days.
- NB! Each person is unique and for this reason symptoms vary.
What next?
- This all depends on what is found during the procedure. All the options will be discussed in detail.
- You may require further attention to your prostate or bladder outlet to prevent further stone formation.
- There may be some blood in the urine. This can be remedied by drinking plenty of fluids until it clears.
- Patients should schedule a follow-up appointment within 1 month to discuss the etiology of the calculus as well as what other procedures may be involved to prevent this from occurring again.
- Please don’t hesitate to direct all further queries to Dr Schoeman.
Download Information Sheet
 Patients will receive a general anaesthesia.
Patients will receive a general anaesthesia.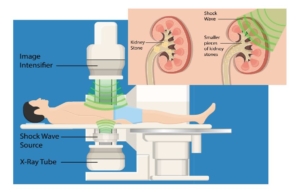
 A General anesthetic will be given.
A General anesthetic will be given.
/Picture35.png)